Mycology Questions with Text (Set 1)
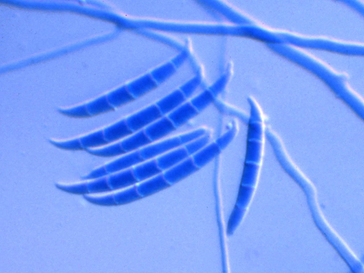
a. Fusarium species
b. Penicillium species
c. Acremonium species
d. Scopulariopsis species
e. Paecilomyces species
a. Phaeohyphomycoses
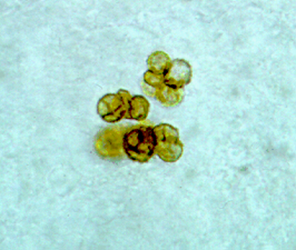
b. Chromoblastomycoses
c. Mycetoma
d. Sporotrichosis
e. Actinomycosis
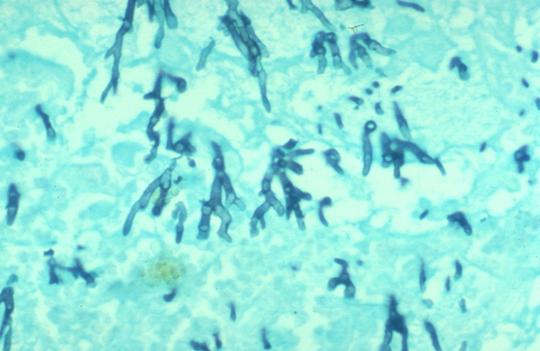
- A lung biopsy from a 50 year-old lung transplant patient revealed uniform hyaline hyphae with regularly spaced septations and branching at a 45 degree angle. No yeast cells were observed. Which of the following is the most probable diagnosis?
a. Actinomycosis
b.Aspergillosis
c. Blastomycosis
d. Cryptococcosis
e. Zygomycosis
4. A 56 year-old female visited her physician because of red nodular and ulcerative painful lesions on her right arm. She recalls being stuck with rose thorns while gardening. A yeast-like colony grew in culture after 5 days of incubation at 30°C. The colony progressively turned black over 7 days. Which organism is the most likely etiology?
b. Candida albicans
c. Nocardia asteroides
d. Sporothrix schenckii
e.Prototheca species
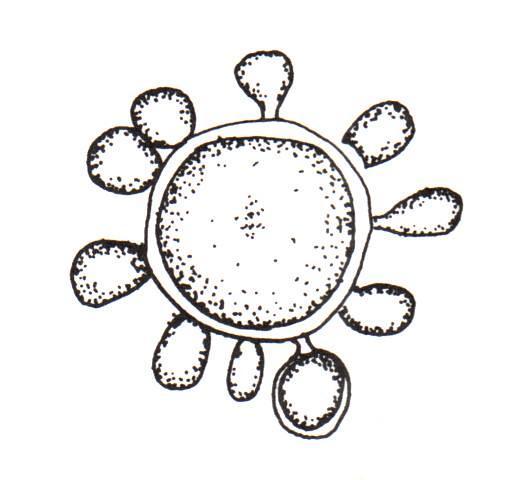
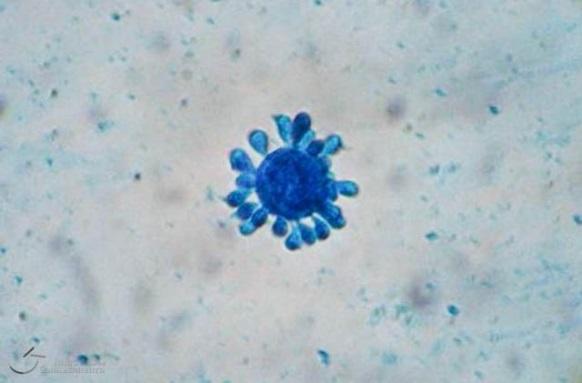
5. A 45 year-old male complained of a slow growing lesion in his nasal cavity. He was a recent immigrant from Brazil. A biopsy of the lesion stained with Gomori Methenamine Stain (GMS) showed a large yeast cell (20 um) with multiple small buds appearing in a “mariners-wheel” type arrangement. Which organisms is the most likely etiology?
a. Blastomyces dermatitidis
b. Paracoccidioides brasiliensis
c. Prototheca species
d. Trichosporon beigelii
e. Cryptococcus albidus
ANSWERS
1. (a) Fusarium is a filamentous fungus widely distributed on plants and in the soil as well as being a common contaminant and a well-known plant pathogen. The genus Fusarium currently contains over 20 species. The most common of these are Fusarium solani, Fusarium oxysporum, and Fusarium chlamydosporum Fusarium is one of the emerging causes of opportunistic mycoses. Fusarium spp. are causative agents of superficial and systemic infections in humans. The most virulent Fusarium spp. is Fusarium solani. Trauma is the major predisposing factor for development of cutaneous infections due to Fusarium strains. Disseminated opportunistic infections, on the other hand, develop in immunosuppressed hosts, particularly in neutropenic and transplant patient. Fusarium infections following solid organ transplantation tend to remain local and have a better outcome compared to those that develop in patients with hematological malignancies and bone marrow transplantation patients.
1. (a) Fusarium is a filamentous fungus widely distributed on plants and in the soil as well as being a common contaminant and a well-known plant pathogen. The genus Fusarium currently contains over 20 species. The most common of these are Fusarium solani, Fusarium oxysporum, and Fusarium chlamydosporum Fusarium is one of the emerging causes of opportunistic mycoses. Fusarium spp. are causative agents of superficial and systemic infections in humans. The most virulent Fusarium spp. is Fusarium solani. Trauma is the major predisposing factor for development of cutaneous infections due to Fusarium strains. Disseminated opportunistic infections, on the other hand, develop in immunosuppressed hosts, particularly in neutropenic and transplant patient. Fusarium infections following solid organ transplantation tend to remain local and have a better outcome compared to those that develop in patients with hematological malignancies and bone marrow transplantation patients.
- (b) Chromoblastomycosis is a mycotic infection of the cutaneous and subcutaneous
Tissues characterized by the development in tissue of dematiaceous (brown-pigmented), planate-dividing, rounded sclerotic bodies. Infections are caused by the traumatic implantation of fungal elements into the skin and are chronic, slowly progressive and localized. Tissue proliferation usually occurs around the area of inoculation producing crusted, verrucose, wart-like lesions. World-wide distribution but more common in bare footed populations living in tropical regions.
Etiological agents include various dematiaceous fungi associated with decaying vegetation or soil, especially Phialophora verrucosa, Fonsecaea pedrosoi, F. compacta and Cladophialophora carrionii Lesions of chromoblastomycosis are most often found on exposed parts of the body and usually start as a small scaly papules or nodules which are painless but may be itchy and as the disease develops rash-like areas enlarge and become raised irregular plaques that are often scaly or verrucose. In long standing infections, lesions may become tumorous and even cauliflower-like in appearance

- (b) Aspergillus.
Although most people are often exposed to Aspergillus, infections caused by the fungus rarely occur in people who have a healthy immune system. The fungus is commonly found growing on dead leaves, stored grain, compost piles, or in other decaying vegetation.
There are several forms of aspergillosis:
Allergic bronchopulmonary type that is an allergic reaction to the fungus. This infection usually develops in people who already have lung problems such as asthma or cystic fibrosis.
Aspergilloma is a growth (fungus ball) that develops in an area of past lung disease or lung scarring such as tuberculosis or lung abscess.
Pulmonary aspergillosis is an invasive type that is a serious infection with pneumonia that can spread to other parts of the body. This infection almost always occurs in people with a weakened immune system due to cancer, AIDS, leukemia, an organ transplant, chemotherapy, or other conditions or medications that lower the number or function of normal white blood cells or weaken the immune system.
The morphology of Aspergillus is better appreciated on special stains such as GMS and shows thin, septate hyphae with regular septations. The angle of the regular branching is at 45 degrees.
- (d) Sporothrix schenkii. In nature Sporothrix lives as a saprophyte on wood, decaying vegetation (including rose thorns), Sphagnum moss, animal excreta and soil. The characteristic infection with Sporothrix involves suppurating subcutaneous nodules that progress along lymphatic channels (lymphocutaneous sporotrichosis). Primary pulmonary infection can occur (although rare) from inhalation of fungal spores (pulmonary sporotrichosis). In rare cases, disseminated S schenckii infection (disseminated sporotrichosis) occurs, characterized by disseminated cutaneous lesions and involvement of multiple visceral organs; this occurs most commonly in persons with AIDS.

- (b) Paracoccidioides brasiliensis
Paracoccidioidomycosis is a chronic granulomatous disease that characteristically produces a primary pulmonary infection, often inapparent, and then disseminates to form ulcerative granulomata of the buccal, nasal and occasionally the gastrointestinal mucosa. The only etiological agent, P. brasiliensis is found in South and Central America. Microscopically, numerous large, 20-60 um, round, narrow base budding yeast cells are present. Single and multiple budding occurs, the latter are thick-walled cells that form the classical "steering wheel" or "Mariners wheel” morphology.
Reference:
Versalovic, J, et al. Fungi, In: Manual of Clinical Microbiology, 10th ed., ASM Press; 2011.
No comments:
Post a Comment