Virology Review Questions
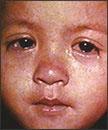
- A 10 year old boy was examined in the emergency room. He had a 24 hour history of fever (101.7*F), runny nose, sore throat, inflamed eyes and skin rash (large blotches). Upon examination inside the mouth, tiny white spots with bluish-white centers were seen This patient’s infection is most likely:
- Varicella –Zoster
- Rubella
- Rubeola
- Enterovirus
- Coronavirus

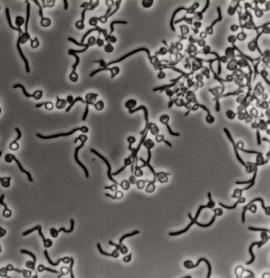
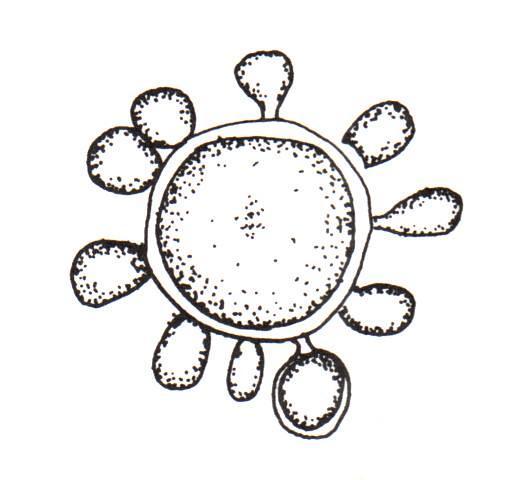
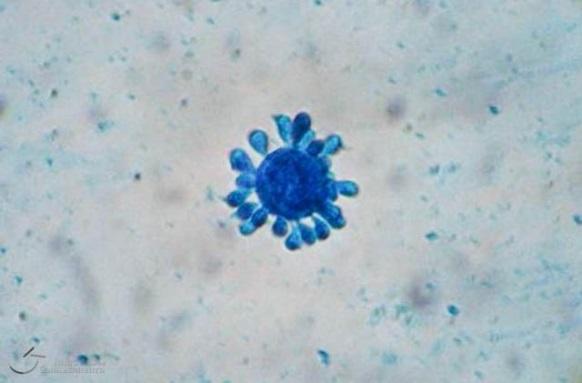
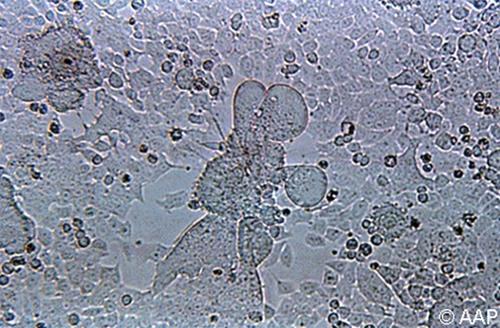
- A one year old boy visited his physician with coughing, sneezing, fever (102°F) and some difficulty breathing. A nasal washing was collected and was sent to the laboratory for testing which included a viral cell culture. The picture below is most consistent with which viral pathogen (Cytopathic effect in Hep-2 cell line):
- Rhinovirus
- Human metapneumovirus
- Coronavirus
- Respiratory Syncytial virus
- Parainfluenzae virus
- A 34 year old female became abruptly ill after arriving home from a three day cruise to Ensenada, Mexico. She developed acute onset of vomiting and developed watery non-bloody diarrhea. She heard that numerous travelers had also become ill following the cruise. She started feeling better twenty four hours after symptoms began. Her disease is most consistent with which pathogen:
- Norovirus
- Rotavirus
- Sapovirus
- Enterovirus
- Astrovirus
- A 40 year old male returned from the Caribbean one week prior. He had a sudden onset of fever (102*F), intense joint pain, headache, and a maculo-papular rash. While in the Caribbean he experirience many mosquito bites. The best diagnostic test should include:
- Viral cell culture of nasal secretions
- IgG, IgM for Dengue virus (serum)
- Qualitative PCR for Chikungunya virus (blood)
- Quantitative PCR for Dengue virus (blood)
- Qualitative PCR for Chikungunya virus (urine)
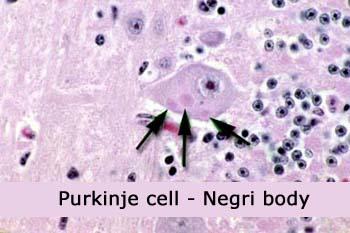
- A 16 year old girl returned from a trip to Mexico approximately one week prior and reported to her local Emergency Department (ED). During her trip she encountered various animals along the way, including feral dogs and cats. She approached a few of the animals and was involved in some skirmishes with small nips and scratches. In the ED, she was found to have general weakness, slight fever and headache for the last few days. Over the next week she progressed to a state of anxiety and confusion and a brain biopsy was performed. This pathology is diagnostic for which infection:
- Cytomegalovirus
- Rabies virus
- Toxoplasmad. Varicella Zostere. Herpes simplex
ANSWERS
- (c) Measles is historically a childhood infection caused by the Rubeola virus. Once quite common, measles can now be prevented with a vaccine (MMR- Measles, Mumps and Rubella). Measles can be serious and even fatal for small children. While death rates have been falling worldwide as more children receive the measles vaccine, the disease still kills more than 100,000 people a year, most under the age of 5. Non-immunized adults are susceptible to infection and can experience complications. Measles signs and symptoms appear 10 to 14 days after exposure to the virus. Signs and symptoms of measles include cough, runny nose, inflamed eyes (conjunctivitis), sore throat, fever and a red, blotchy skin rash. The skin rash is made of large, flat blotches that often flow into one another. Also seen are tiny white spots with bluish-white centers on a red background found inside the mouth on the inner lining of the cheek — known as Koplik's spots. If laboratory diagnosis is necessary the tests of choice include serum IgM for measles antibody and qualitative PCR on a urine specimen.
- (d) Respiratory Syncytial Virus (RSV) causes infections of the lungs and respiratory tract. It's so common that most children have been infected with the virus by age 2. Respiratory syncytial virus can also infect adults. In adults and older, healthy children, the symptoms of respiratory syncytial virus are mild and typically mimic the common cold. Self-care measures are usually all that's needed to relieve any discomfort. Infection with respiratory syncytial virus can be severe in some cases, especially in premature babies and infants with underlying health conditions. RSV can also become serious in older adults, adults with heart and lung diseases, or anyone with a very weak immune system (immunocompromised). If laboratory testing is necessary, currently the most useful test is polymerase chain reaction using nasopharyngeal or nasal secretions (PCR). In years past, viral cell culture was the method of choice. The presence of RSV is confirmed by the formation of giant cells or syncytia formation in inoculated cell cultures in 1 – 2 weeks.
- (a) Noroviruses are a group of viruses that cause inflammation of the stomach and large intestine lining (gastroenteritis); they are the leading cause of gastroenteritis in the U.S. The norovirus was originally called the Norwalk virus after the town of Norwalk, Ohio, the location of the first confirmed outbreak in 1972. People become infected with noroviruses when they eat food or drink liquids that have been contaminated. You can also become infected if you touch an object or surface that has been infected with the virus and then touch your nose, mouth, or eyes. Noroviruses thrive on cruise ships (as well as in day-care centers, restaurants, nursing homes, and other close quarters) because they are very hardy and highly contagious. They can survive temperature extremes in water and on surfaces. Once someone is infected from contaminated food, the virus can quickly pass from person to person through shared food or utensils, by shaking hands or through other close contact. People who have a weakened immune system are particularly susceptible to catching noroviruses, When infected with norovirus, you will be ill within a 24-48 hours with nausea, vomiting (more often in children), watery diarrhea (more often in adults), and stomach cramps. If diagnostic testing is necessary, this virus cannot grow in cell culture and the method of choice is polymerase chain reaction (PCR) on stool or vomitus.
- (c) Chikungunya is a viral disease that is transmitted by mosquitoes. It has occurred in Africa, Southern Europe, Southeast Asia, and islands in the Indian and Pacific Oceans, In late 2013. Chikungunya was found for the first time in the Americas on islands in the Caribbean. Aedes species mosquitoes transmit chikungunya virus and this is the same genus of mosquitoes that transmit dengue virus. These mosquitoes bite mostly during the daytime. Symptoms usually begin 3‒7 days after being bitten by an infected mosquito and the most common symptoms are fever and severe joint pains, often in the hands and feet. Other symptoms may include headache, muscle pain, joint swelling, or rash. Unlike Dengue, there are no hemorrhagic complications. There are no antiviral medicines to treat chikungunya. Most patients improve after 7 days. People at increased risk for severe disease include newborns exposed during delivery, older adults (≥65 years), and people with medical conditions such as high blood pressure, diabetes, or heart disease, but deaths are rare.
- (b) Rabies virus belongs to the family Rhabdovirid and have a distinct "bullet" shape that can be seen on EM. The first symptoms of rabies may be very similar to those of the flu including general weakness or discomfort, fever, or headache. These symptoms may last for several days. There may be also discomfort or a prickling or itching sensation at the site of bite, progressing within days to symptoms of cerebral dysfunction, anxiety, confusion, agitation. As the disease progresses, the person may experience delirium, abnormal behavior, hallucinations, and insomnia. The acute period of disease typically ends after 2 to 10 days. Once clinical signs of rabies appear, the disease is nearly always fatal, and treatment is typically supportive. Disease prevention includes administration of both passive antibody, through an injection of human immune globulin and a round of injections with rabies vaccine. Histopathologic evidence of rabies encephalomyelitis (inflammation) in brain tissue and meninges includes the following: Mononuclear infiltration, Perivascular cuffing of lymphocytes or polymorphonuclear cells, Lymphocytic foci, and Negri bodies.
References:
Centers for Disease Control and Prevention, CDC Home site.
Manual of Clinical Microbiology, 10th Edition, 2011. Editors: James Versalovic1, Karen C. Carroll2, Guido Funke3, James H. Jorgensen4, Marie Louise Landry5, David W. Warnock